Strong bones support the body, but bone density declines with age and hormonal changes. With the right approach, we can maintain strength and reduce fracture risk.
As an Endocrinologist and ISCD-certified clinical densitometrist, I’d like to share how.
-Anna Groysman MD, MSCP, CCD

Bone Health Site Index

What is Osteoporosis and Osteopenia?
Osteoporosis and osteopenia are both conditions involving lower-than-normal bone density, with osteopenia being the milder precursor and osteoporosis the more severe form
How Common is Osteoporosis?
30% of women age 65 and older have osteoporosis.
An additional 40% of postmenopausal women have osteopenia

Why You Should Protect Your Bone Density
“According to recent statistics from the International Osteoporosis Foundation, worldwide, 1 in 3 women over the age of 50 years and 1 in 5 men will experience osteoporotic fractures in their lifetime.”
What happens after a hip fracture?
Only 50% of women recover their ability to perform daily activities (like bathing, dressing, and walking) within 6 months.
Only 25% recover their ability to perform more complex tasks (like shopping, cooking, and managing finances)
Women are 5 times more likely to need nursing home placement within one year after a hip fracture compared to women who haven't had a fracture
Mortality Risk
The risk of death doubles within the first year after a hip fracture
About 24% die within one year
Why do I sound like a “Debbie Downer” when I share these statistics? Because they are real—and they affect real women. My goal is to ensure my patients are well-informed, so they can make thoughtful decisions and take proactive steps to protect their health.


-
A DXA scan (bone density test) is a quick, painless way to check your bone health. It’s similar to a regular X-ray, but measures the strength and mineral content of your bones instead of just taking pictures of them. DXA scans are used to screen you for osteoporosis, osteopenia and other conditions that can silently weaken your bones.
-
DXA scans are outpatient procedures, which means you won’t have to stay in the hospital. There are no needles or injections in this test, and you won’t feel any pain.
You might be able to wear your regular clothes during the test, or you may have to change into a hospital gown.
-
A bone density test usually lasts around 30 minutes. Your test might be slightly shorter or longer depending on how many of your bones need scanning
-
A standard DXA scan delivers an effective dose roughly equivalent to 1-2 days of natural background radiation, making it one of the lowest-dose medical imaging procedures available.
Bone Mineral Density Test (BMD) or DXA Scan

Nutrition for Stronger Bones
Protein: Protein is necessary to build and repair bones and to keep muscles strong. When muscles are strong, our balance and movement is optimally supported. Diets that include recommended amounts of protein are associated with greater bone mass and fewer fractures when calcium intake is adequate. Adults with limited protein intake are at high risk for bone loss and fractures.
Magnesium - Magnesium helps convert vitamin D into its active form, which in turn helps us absorb calcium. The recommended daily magnesium intake for women ≥ 50: 320mg daily and for men ≥ 50: 420mg daily.
Magnesium is found in many foods, particularly in plant-based food sources.
Most people will not need a magnesium supplement to meet their daily magnesium nutritional goals.
Here are foods rich in magnesium:
Leafy green vegetables: spinach, Swiss chard, kale
Nuts and seeds: almonds, cashews, pumpkin seeds, chia seeds, flaxseeds
Legumes: black beans, chickpeas, lentils, edamame
Whole grains: brown rice, quinoa, oats, whole wheat
Fish: salmon, mackerel, halibut
Avocados
Dark chocolate (70% or higher cocoa)
Bananas
Tofu and soy products
Dairy: milk and yogurt (moderate amounts)
Vitamin K: Vitamin K activates a protein that helps build bone.
Vitamin K is widely available in plant and animal-based food sources. Most people will not need to take supplements to get enough vitamin K .
Daily recommended vitamin K intake in women ≥ 50: 90mcg and in men ≥50: 120mcg.
Here are foods rich in vitamin K:
Leafy green vegetables (highest sources): kale, spinach, collard greens, Swiss chard, mustard greens, turnip greens
Cruciferous vegetables: broccoli, Brussels sprouts, cabbage
Herbs: parsley, basil, cilantro
Vegetable oils: soybean oil, canola oil
Green vegetables: green beans, asparagus, peas
Fermented foods: natto (very high in vitamin K2)
Animal sources (smaller amounts of K2): egg yolks, liver, cheese
People on warfarin should avoid vitamin K supplementation as it interferes with its blood thinning effect.
Vitamin D: A target vitamin D level of ≥30 ng/mL is recommended. This is often achieved with 400–1000 IU of vitamin D daily, though individual needs vary based on absorption. Dosing should be adjusted to maintain a blood level above 30 ng/mL.
Calcium: This is the primary mineral responsible for bone strength. The recommended intake for adults is 1,200 mg of calcium daily. I recommend getting most of this from food, and using a supplement only on days when dietary intake falls short of 1,200 mg.
Calcium citrate is preferred if you are taking acid-suppressing medications such as famotidine, pantoprazole, or omeprazole, and it can be taken with or without food.
Calcium carbonate, on the other hand, should be taken with food to improve absorption.
Calcium supplements may increase the risk of kidney stones.
Your calcium needs may differ if you have conditions such as chronic kidney disease or hyperparathyroidism or a history of gastric bypass surgery.

Exercise

What Kind of Exercise Will Have a Better Impact?
I encourage you to stay active and include weight-bearing activities in your daily routine—such as standing, walking, safe gardening, or shopping. Remember that the four pillars of preventing frailty include muscle strengthening, balance training, cardiovascular exercises that increase heart rate, and stretching.
~Anna
Weight-bearing and resistance exercises are crucial for bone health because they provide the mechanical loading forces that stimulate bone formation and help slow bone loss.
Exercise can reduce fracture risk by about 10% through improved bone strength and by reducing fall risk through enhanced balance and muscle strength.
Please consult your physician and/or physical therapist before starting any exercise program. Exercise should be individualized so it can be tailored to your needs — maximizing both safety and benefit based on your physical abilities.
If you are a beginner, Dr. Groysman created a simple to follow exercise program video for people who are looking to start, but don’t know how.
High-impact weight-bearing exercises: Activities that generate ground reaction forces greater than walking alone
Recommend most days of the week for at least 30 minutes
Jogging
Stair climbing
Tennis
Dancing
Jumping activities
Low-impact weight-bearing exercises: These activities offer a safe alternative for individuals who cannot perform high-impact exercise, such as those with a history of vertebral fractures or multiple low-trauma fractures.
Brisk walking
Hiking on level ground - Some use hiking poles to improve their balance, click below for more information
Low-impact aerobics
Muscle-Strengthening Exercises: Moving against resistance
2-3 times per week involving 2-3 sets of 8-12 repetitions maximum targeting major muscles
Weight training
Lifting your own body weight: squats, lunges
Elastic exercise bands
Balance and Back Extension Exercises: These improve posture, reduce fall risk, and may help prevent vertebral fractures. Working on balance is important because approximately 95% of hip fractures result from falls. You should consider the following exercises to improve balance:
Tai chi
Leaning forward, backward, or side to side
Unusual walking - such as walking heel-to-toe or reacting to things that make you change directions
Yoga
Back extension exercises
Want To Learn More?
Please Click the Link Below to Download a Comprehensive Exercise handout from the Canadian Society of Osteoporosis


Moving Safely
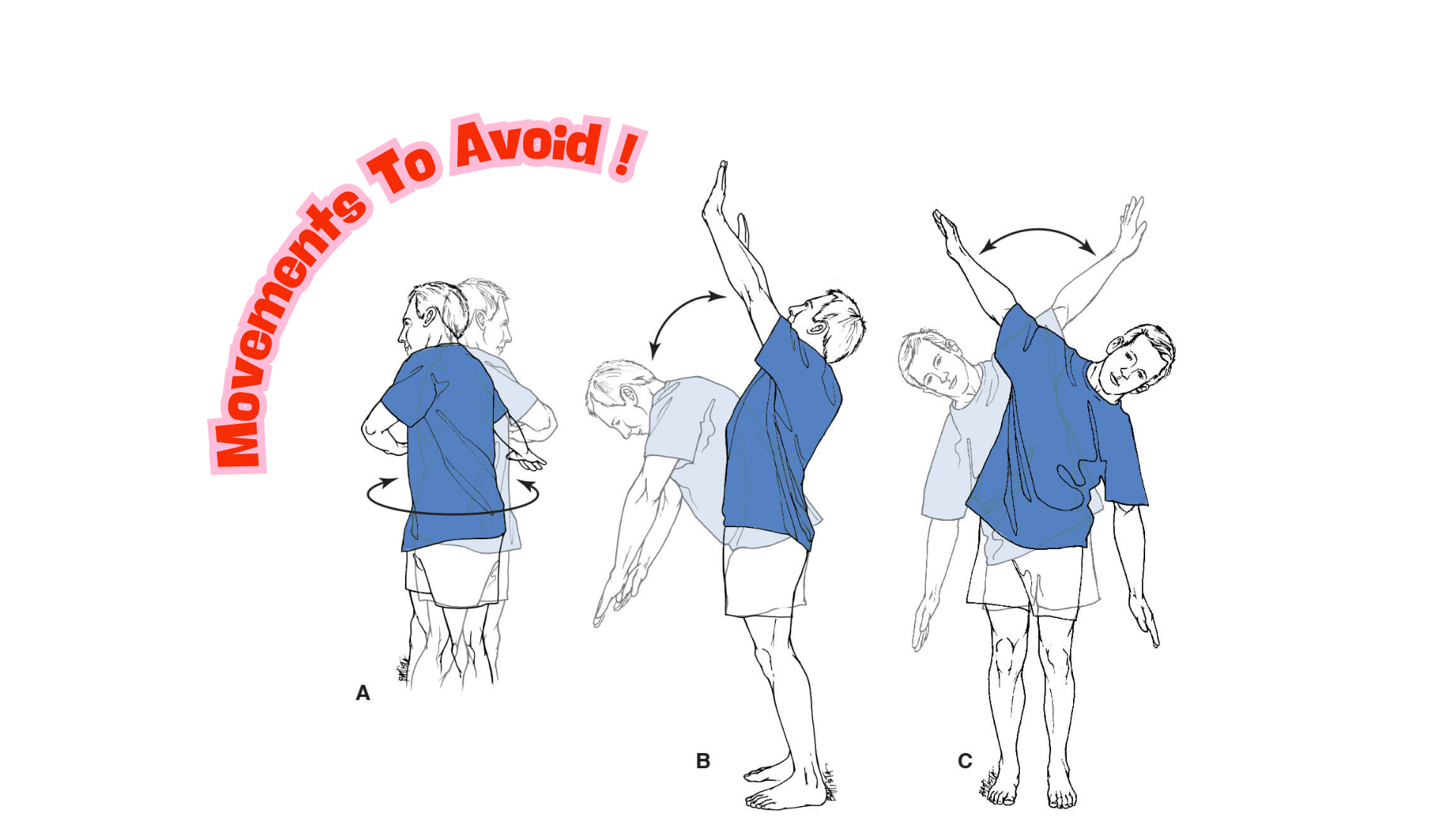
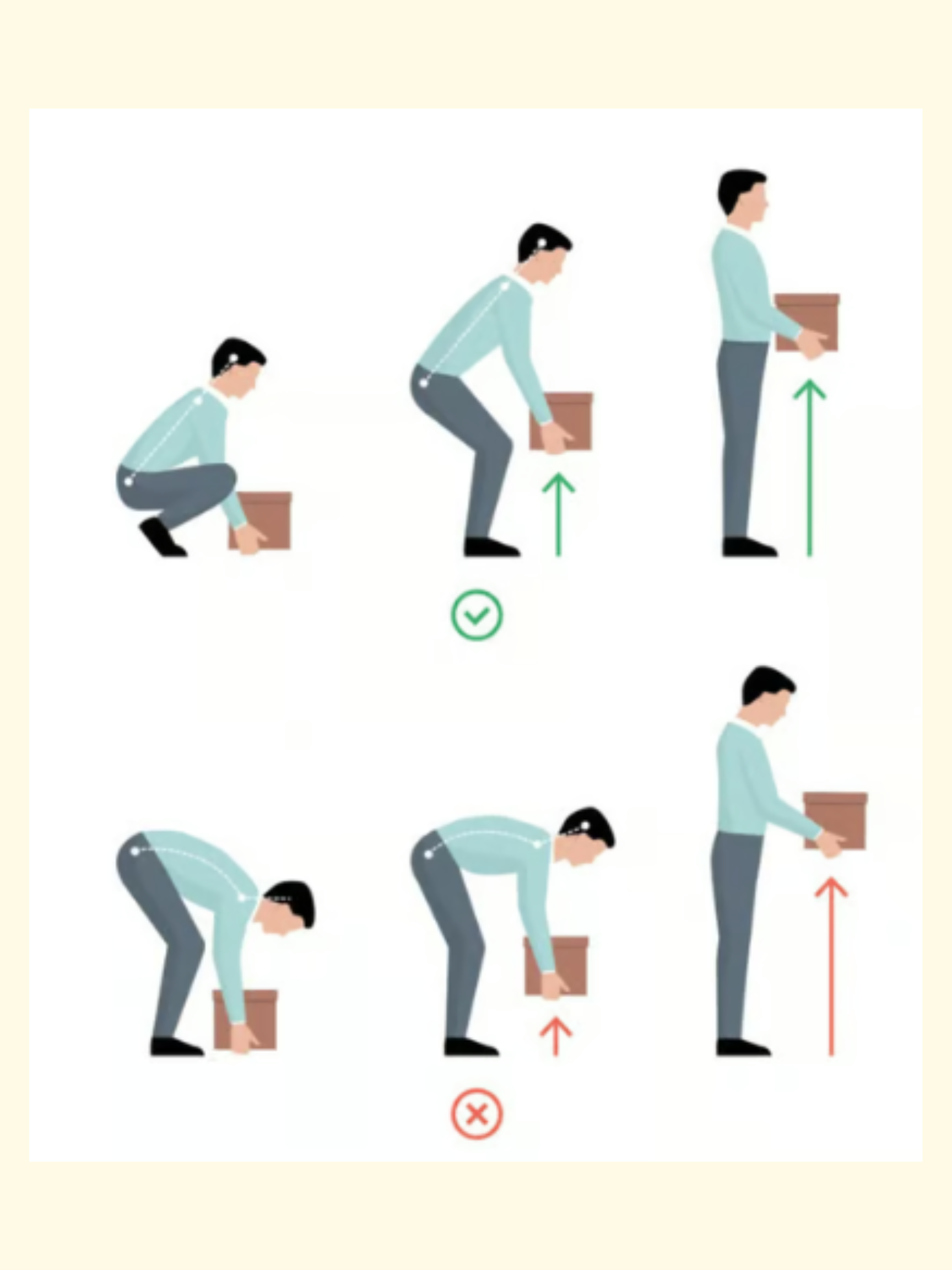
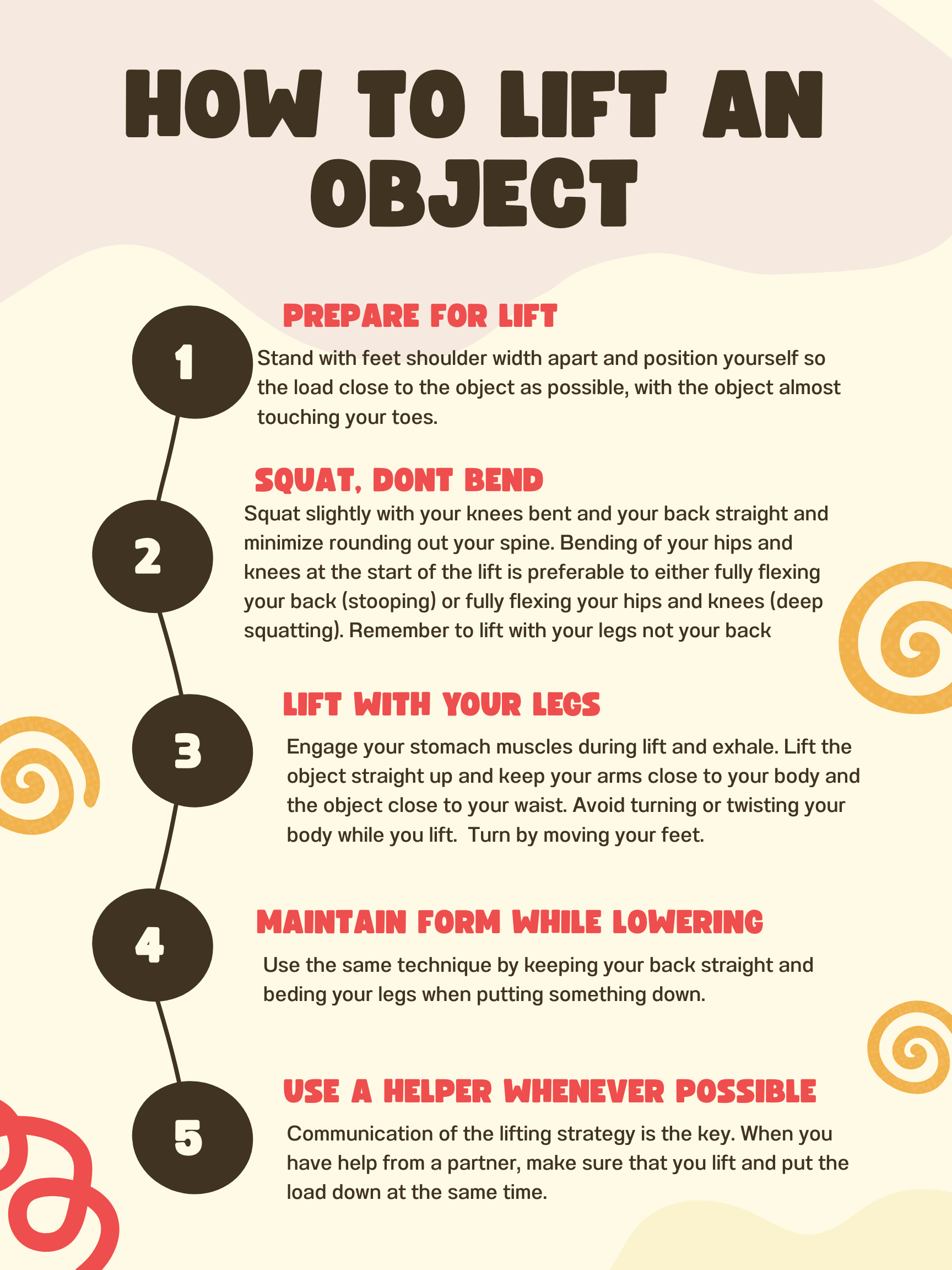
Individuals with severe osteoporosis or vertebral fractures should avoid exercises involving high degrees of spinal flexion (forward bending), twisting, or side bending, as these can exert compressive forces that may lead to fracture.
People at high risk of fracture may need to limit repetitive bending, twisting, holding a bent or twisted position for an extended period of time.

Reducing Fall Risk
Age is important when it comes to your risk of osteoporosis. As women approach menopause, bone loss occurs at an increased rate. Men start to have increased bone loss at 65+.
A significant family history of osteoporosis is linked to a higher likelihood of developing the condition. If your parent had a hip fracture, it may indicate an increased risk for you in osteoporosis and future fractures.
What happens if you fracture?
By definition, this is considered severe osteoporosis unless the fracture occurred from a traumatic event, such as a car accident or a fall from a significant height. A fracture may be the first and only sign of osteoporosis. The greatest risk factor for a repeat fracture is a prior fracture.
It is possible to reduce your risk of another fracture.
You should see a physician who understands how to manage osteoporosis. You do not need to wait for a bone density test, but you do need to start treatment with a bone-building medication as soon as possible.
The Center of Disease Control (CDC) created a free handout to check your home for safety and prevent potential falls. You can download a free PDF by clicking the link below.


Smoking has negative consequences on your bone health. This is a reminder to Quit.
Reduce Alcohol Intake to Less than 2 Drinks Per Day. Abstinence is preferred.

Weighing the risk of treating vs. not treating osteoporosis with medications
Unfortunately, lifestyle measures are not enough to prevent fractures once a person is diagnosed with osteoporosis. At this point, medications in combination with lifestyle changes are needed to accomplish this goal.
Many of my patients are hesitant to start medications mainly because they are concerned about the risk of osteonecrosis (rotting) of the jaw or atypical hip fractures that are known side effects.
However, I want to take a moment to discuss the EXTENT of risk from treatment compared to EXTENT of risk from not being treated.
What is the risk of not treating osteoporosis?
People with osteoporosis are at a high risk of fracture. Hip fracture outcomes are devastating. Within 1 year, up to 30% of people with a fracture will die. The risk of death remains double. Up to 75% of people do not recover their pre-fracture ambulatory or functional status by one year. Up to 20% of people who sustain a fracture require transition to a long-term care facility within the first year.
What is at stake includes your physical function, independence, and overall risk of death.
What are the risks of treatment?
For the most common medications like reclast and fosamax (alendronate), the risks are as follows:
Osteonecrosis of the Jaw
This is a rare condition where a portion of the bone loses its blood supply and begins to die. Typically, we give breaks or “drug holidays” to reduce the risk of this occuring.
The risk is (0.017%) 1.7 cases per 10,000 patients after 3 years of yearly therapy with no increase in risk through 6 years of treatment. This is similar to the risk of dying from a bee sting.
The risk is higher with poor dental hygiene, dental extraction or invasive dental procedure, smoking, and prolonged use of medication.
Atypical hip Fracture
This is a rare type of fracture that occurs at the thigh bone just below the hip after minimal trauma. It occurs from long-term use of certain bone medications. Typically, we give breaks or “drug holidays” to reduce the risk of this occurring.
The risk is extremely low- estimated at 1 case per 1,000 to 10,000 patient years, depending on duration of use.
Most cases occur after long term use of osteoporosis medications
The absolute risk of medication side effects, even with prolonged use, is far outweighed by the fractures prevented. We use drug holidays strategically to minimize any potential risks from treatment. What I see far more often in practice are fractures in patients who weren't treated—fractures that could have been avoided. Side effects are the exception; preventable fractures are not.

Common Medications for Osteoporosis
Osteoporosis medications help strengthen your bones and reduce your risk of fractures. Below is a summary of the most common medications used to treat osteoporosis.
Zoledronic Acid (Reclast)
How it works: Slows down the cells that break down bone (osteoclasts), allowing your bones to stay stronger.
How it's given: Intravenous (IV) infusion at your doctor's office or infusion center.
How often: Once a year.
Common side effects:
Flu-like symptoms (fever, muscle aches, headache) for 1-3 days after infusion (up to 30% of patients, usually only after the first dose)
Temporary mild increase in creatinine (kidney marker)
Rare side effects:Osteonecrosis of the jaw (ONJ) and atypical femur fracture (AFF)—see "Rare but Serious Side Effects" section below.
Who should NOT take this medication:
Kidney disease (creatinine clearance less than 35 mL/min)
Low calcium levels
Allergy to bisphosphonates
Oral Bisphosphonates (Alendronate/Fosamax, Risedronate/Actonel)
How it works: Same as zoledronic acid—slows bone breakdown.
How it's given: Pill taken by mouth on an empty stomach with a full glass of water. You must stay upright (sitting or standing) for at least 30 minutes afterward and not eat or drink anything else during that time.
How often:
Alendronate: 70 mg once weekly
Risedronate: 35 mg once weekly or 150 mg once monthly
Common side effects:
Heartburn, stomach upset, or difficulty swallowing (20-30% of patients)
Muscle or joint aches (about 4% of patients)
Rare side effects:Osteonecrosis of the jaw (ONJ) and atypical femur fracture (AFF)—see "Rare but Serious Side Effects" section below.
Who should NOT take this medication:
Kidney disease (creatinine clearance less than 30-35 mL/min)
Esophagus problems (such as difficulty swallowing, esophagitis, or ulcers)
Inability to stay upright for 30 minutes
Low calcium levels
Denosumab (Prolia)
How it works: Blocks a protein (RANKL) that activates bone-breakdown cells, reducing bone loss.
How it's given:Injection under the skin, usually given in your doctor's office.
How often: Every 6 months. It is very important not to miss or delay doses.
Common side effects:
Skin reactions (eczema, rash) in about 3% of patients
Skin infections (cellulitis) in less than 1% of patients
Rare side effects: Osteonecrosis of the jaw (ONJ) and atypical femur fracture (AFF)—see "Rare but Serious Side Effects" section below.
Important note: If you stop this medication without transitioning to another specific osteoporosis treatment, there is a risk of rapid bone loss and rebound vertebral fractures. You must transition to another medication (usually a bisphosphonate) before or shortly after stopping Prolia. Never stop this medication without talking to your doctor first.
Who should NOT take this medication:
Low calcium levels
Allergy to denosumab
Romosozumab (Evenity)
How it works:Blocks a protein called sclerostin, which both builds new bone AND slows bone breakdown—a dual action.
How it's given:Two injections under the skin (given at the same visit), usually in your doctor's office or at an infusion center administered by a nurse.
How often:Once a month for 12 months only.
Common side effects:
Injection site reactions (about 5% of patients)
Joint pain, headache, muscle pain
Important warnings:
May increase risk of heart attack, stroke, or cardiovascular death
After completing 12 months, you must continue with another osteoporosis medication
Who should NOT take this medication:
Heart attack or stroke within the past year
Low calcium levels
Allergy to romosozumab
Teriparatide (Forteo) and Abaloparatide (Tymlos)
How they work: Stimulate bone-building cells (osteoblasts) to create new bone—these are "anabolic" or bone-building medications.
How they're given: Daily self-injection under the skin using a pen device (similar to insulin pens).
How often:
Teriparatide: 20 micrograms daily
Abaloparatide: 80 micrograms daily
Duration: Limited to 18-24 months total lifetime use.
Common side effects:
Nausea (about 20% of patients)
Headache (about 13% of patients)
Dizziness or lightheadedness
Leg cramps (about 3% of patients)
Mildly elevated calcium levels (3-6% of patients)
Important note:After completing treatment, you must continue with another osteoporosis medication (usually a bisphosphonate or denosumab) to maintain bone gains.
Who should NOT take these medications:
Kidney disease (creatinine clearance less than 30 mL/min)
History of bone cancer or radiation therapy to bones
Paget's disease of bone
High calcium levels
Unexplained elevated alkaline phosphatase
Rare but Serious Side Effects
The following rare side effects can occur with some osteoporosis medications. While the risk is very low, it is important to be aware of them:
Osteonecrosis of the jaw (ONJ):
A rare condition where part of the jawbone doesn't heal properly, usually after dental procedures
Risk is very low: less than 1 in 10,000 to 1 in 1,000 patients (0.01-0.1%)
Can occur with: bisphosphonates (Reclast, Fosamax, Actonel), denosumab (Prolia), and romosozumab (Evenity)
Prevention: Maintain good dental hygiene, have regular dental checkups, and inform your dentist about your medication before any dental procedures
Atypical femur (thigh bone) fracture (AFF):
A rare type of fracture in the thigh bone that can occur with minimal or no trauma
Risk is very low: about 1-2 per 10,000 patients per year, but increases with longer duration of treatment
Can occur with: bisphosphonates (Reclast, Fosamax, Actonel) and denosumab (Prolia)
Warning sign: New or unusual pain in your thigh or groin—report this to your doctor immediately
Risk decreases after stopping the medication
Rebound fractures after stopping Prolia (denosumab):
If Prolia is stopped without transitioning to another osteoporosis medication, bone density can drop rapidly—sometimes below pre-treatment levels
This can lead to multiple vertebral (spine) fractures, sometimes within months of the last dose
This is preventable: always transition to another medication before or shortly after stopping Prolia
Severe low calcium (hypocalcemia):
Can occur with denosumab (Prolia) and romosozumab (Evenity) usually in people with chronic kidney disease
Symptoms may include muscle spasms, twitching, cramps, numbness, or tingling
Prevention: Take calcium and vitamin D supplements as directed and have calcium levels checked before each dose
Cardiovascular events (heart attack, stroke):
Romosozumab (Evenity) may increase the risk of heart attack, stroke, or death from cardiovascular causes
It is important to note that in the ARCH study where romosozumab was compared to alendronate there was a higher incidence of cardiovascular events (1.5% vs 1.9%), leading to the FDA black-box warning. However, this difference was not observed in the FRAME trial where romosozumab was compared to placebo. The conflicting data had generated ongoing debate. A 2020 metanalysis of randomized controlled trials by Lv et al., found no significant increase in cardiovascular risk from Evenity.
This medication should not be used in patients who have had a heart attack or stroke within the past year
Osteosarcoma (bone cancer):
In animal studies, teriparatide (Forteo) and abaloparatide (Tymlos) were associated with bone tumors
This has NOT been confirmed in humans, but as a precaution, these medications are limited to 18-24 months of lifetime use
These medications should not be used in patients with a history of bone cancer, Paget's disease, or prior radiation to the bones
Putting Risk in Perspective
While the rare side effects listed above sound concerning, it is important to understand that the risk of these side effects is very low compared to the risk of fractures from untreated osteoporosis. For example, for every 10,000 patients treated with bisphosphonates for 3 years, approximately 150 hip fractures are prevented while only about 2 atypical femur fractures may occur. Side effects from these medications are extremely rare, but fractures from untreated osteoporosis are common—and most importantly, preventable.
General Recommendations
Take calcium (1,000-1,200 mg daily from food and supplements) and vitamin D (800-1,000 IU daily or as directed) unless your doctor advises otherwise.
Maintain good dental hygiene and have regular dental checkups.
Report any new thigh or groin pain to your doctor.
Do not stop your medication without talking to your doctor first.
If you have questions about your osteoporosis treatment, please discuss them with your clinician.
Additional Questions
Can a Weighted Vest support Bone Density?
The evidence on weighted vests for bone density is mixed and context-dependent. Weighted vests may help prevent age-related bone loss in weight-stable adults when combined with regular exercise. The benefit likely requires consistent exercise while wearing the vest, NOT passive wear time.
Can whole body vibration support Bone Density?
Whole-body vibration (WBV) therapy shows modest but significant benefits for bone mineral density (BMD), particularly in postmenopausal women, though the effects are small and depend on specific vibration parameters (vibration type, frequency, magnitude, cumulative dose). The most consistent evidence supports improvements in lumbar spine BMD in postmenopausal women, with several meta-analyses showing statistically significant increases. The effects on the hip are more variable. WBV is time intensive. Usually requiring 3 sessions per week, 15-20 minutes per session for 6-12 months. Cost can be $2,000-$10,000+