
Peri/Menopause
Page Index

Introduction
Puberty Was Lesson One… This Is Lesson Two
In high school, we got the classic (and slightly awkward) “birds and the bees” talk. There was a surprising amount of excitement around getting your first period—like it was some big milestone you were supposed to celebrate. But then… nothing. No one mentioned what happens later. It was as if once you figured out puberty, you were set for life.
Fast forward a few decades, and suddenly there’s this phase—perimenopause—that sneaks in quietly, without warning. No big announcement, no clear roadmap. Just a slow build of symptoms that can leave you wondering, “What is happening to me?” Many women spend years trying to piece it together, often seeing multiple doctors before getting real answers or relief.
It makes you wonder—why weren’t we taught this part too? Women’s health education shouldn’t stop at puberty. Herein, I discuss this next chapter—what to expect, how to recognize the signs, and how to feel like yourself again.
For ease, I will refer to perimenopause and menopause as peri/menopause

What is Perimenopause and Menopause?
Menopause
Menopause is a normal and natural biological milestone that marks the permanent cessation of a woman’s menstrual cycles. If is officially diagnosed after 12 consecutive months without a menstrual period.
In the United States, the mean age of menopause is 51 but it typically ranges from mid-40s to mid 50s. It can occur earlier in life, however.
Menopause is NOT a disease-it is a normal transition. HOWEVER, it often comes with uncomfortable changes that result in women feeling “not like themselves.”
Menopause is diagnosed retrospectively, based on 12 consecutive months of the absence of a menstrual period.
For women who are on an IUD, had an endometrial ablation, or had a hysterectomy and are no longer bleeding, it can be helpful to check an FSH and estradiol level.
FSH ≥ 40 combined with a low estradiol (less than 20 pg/mL), measured at least 3 months apart, can help orient toward a menopausal diagnosis.
Perimenopause
Perimenopause is the transitional stage before menopause, which can start as early as 10 years before the final menstrual period. It most commonly begins in a woman’s early to mid-40s, though it may start earlier for some.
During this time, the ovaries no longer produce estrogen in a steady, predictable cycle. Instead, hormone levels fluctuate significantly, and this hormonal variability—not just declining estrogen—drives many of the symptoms women notice. Menstrual cycles may become irregular, with bleeding that is heavier, lighter, or more spaced out than usual. Ovulation also becomes less predictable. Despite these changes, pregnancy is still possible during perimenopause.
Perimenopause is characterized by unpredictable hormonal fluctuations.
Estrogen levels can rise and fall erratically
A single lab test only reflects one moment in time—failing to capture the ongoing shifts that often drive symptoms.
Progesterone levels generally decline, but may vary due to irregular and inconsistent ovulation.
Follicle-stimulating hormone (FSH) levels can also change from cycle to cycle, and overall hormone levels may fluctuate significantly from day to day.
For this reason, a single blood draw provides only a snapshot—not the full picture. A thorough clinical history remains the most important tool in diagnosing perimenopause.
Laboratory testing should be considered in some cases when we need to exclude other causes for absence of periods or symptoms. This includes thyroid disorders, pituitary issues, premature ovarian insufficiency in younger women, or polycystic ovarian syndrome.
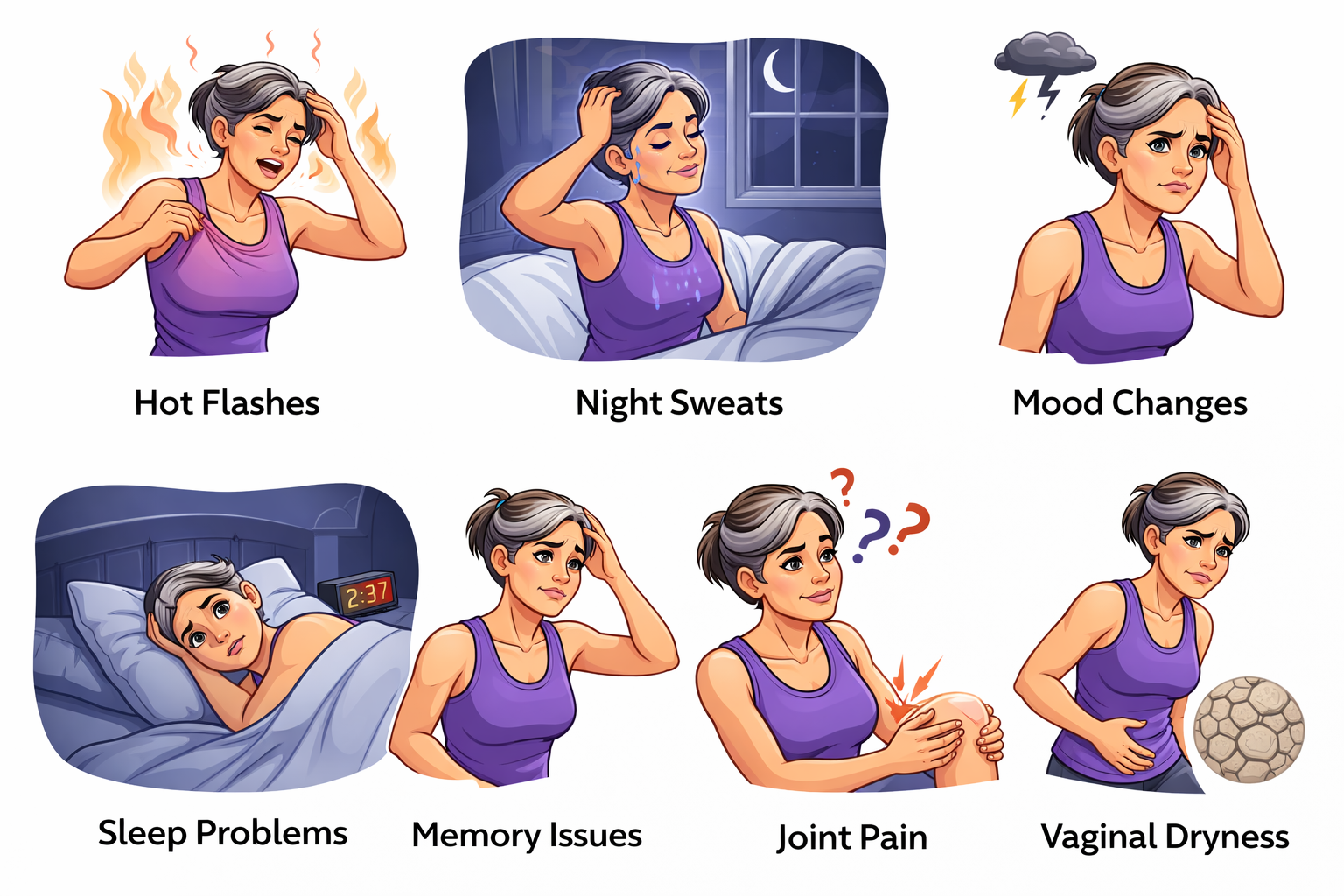
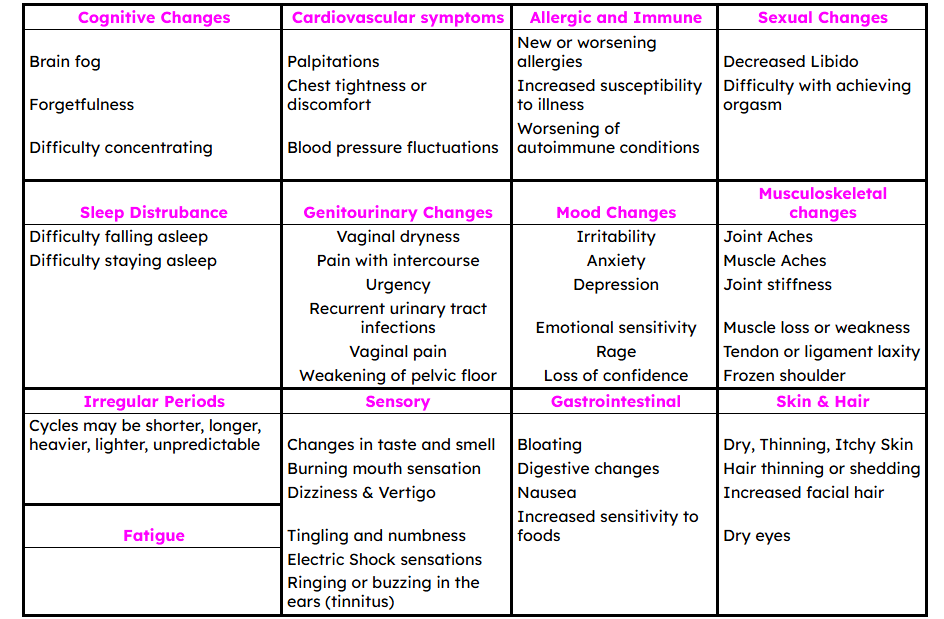
What are the Symptoms of Peri/Menopause?
Perimenopause and menopause can impact nearly every system in the body, and symptoms can differ greatly between women. While some women experience only mild or minimal changes, others may have symptoms that significantly affect their daily life and overall well-being.
The list below includes the most common symptoms, but it is not exhaustive. Please note that not all symptoms are caused by peri/menopause, and it is important not to assume every symptom is related to hormonal changes.

Changes in Peri/Menopause that are silent
Peri/menopause may cause many uncomfortable symptoms. Many women think they are “done with peri/menopause” once hot flashes resolve. I urge you to think again! Estrogen affects almost every part of our body-our skeleton, heart, joints, brain, pelvic floor, gastrointestinal system. For this reason, I am very careful to look at the entire person and all around health.
Let me explain:
Heart: During peri/menopause, women may notice that their blood pressure and cholesterol begin to rise, even without changes in lifestyle. After menopause, cardiovascular events become the leading cause of death in women. Peri/menopause is a critical time to pay close attention to your heart health and monitor cardiac markers.
Bone: Women can lose up to 20% of their bone density during the menopause transition—a significant decline. Although the rate of loss slows after menopause, bone loss continues over time and can lead to osteoporosis, with approximately 1 in 2 women experiencing a fracture in their lifetime. Rather than waiting for osteoporosis to develop, bone density screening and targeted lifestyle interventions can help prevent it.
Metabolic Health: Women may notice that their metabolism changes and that they gain weight despite no changes in lifestyle. Insulin resistance may worsen, and some may develop prediabetes or diabetes. This is a critical time to slow or reverse these changes. Overweight and obesity are not your fault, but they are medical conditions that require attention, just like stroke, seizures, and high cholesterol. Improving weight can, in turn, improve insulin sensitivity and reduce the risk of cancers, joint issues, fatty liver disease, stroke, heart disease, and more.
Muscle loss: With the decline in estrogen, there is an accelerated loss of muscle strength. Over time, this can lead to frailty and weakness. This is a critical time to preserve and strengthen muscle in order to maintain independence later in life. My goal for when I become a senior is that if I fall, I can get up independently and avoid fractures. It is important to work on this proactively.
Joint Changes: More than 50% of women experience muscle or joint pain during peri/menopause. Estrogen receptors are present in both tendon and joint tissue, and estrogen plays an important role in tendon structure and collagen production. As estrogen declines, this can lead to cartilage thinning, increased inflammation, and reduced resilience and repair capacity of connective tissues.
Pelvic changes: With a reduction in estrogen, women may develop vaginal dryness. Over time, these changes can lead to vaginal atrophy, alterations in vaginal pH, and a shift in the healthy bacteria that colonize the vagina. As a result, women are more likely to develop recurrent vaginal infections. This can become a significant problem with age, as it may lead to hospitalizations and can, in some cases, be life-threatening.

What Labs Should be Checked When Evaluating Peri/Menopause?

The menopausal transition is more than just a reproductive milestone—it’s a whole-body shift. Hormone changes can affect cholesterol, blood sugar, bone density, and body composition. Heavy periods can drain iron, and overlooked nutrient deficiencies can make symptoms worse.
That’s why I don’t just treat symptoms—I take a broader approach and screen for the common issues that can develop or worsen during this time.
Heart Health
Estrogen has a protective effect on the cardiovascular system, and its decline during menopause shifts the lipid profile in an unfavorable direction. I evaluate:
Lipid Panel — to assess overall cholesterol, LDL, HDL, and triglycerides
Lipoprotein(a) — a genetically determined marker of cardiovascular risk
Apolipoprotein B (ApoB) — a more precise marker of plaque-forming particles than standard LDL alone
High-Sensitivity CRP (Cardiac-Specific) — to assess systemic inflammation, an independent risk factor for cardiovascular disease
Thyroid Function
Thyroid disorders are common in women and can closely mimic or worsen menopausal symptoms such as fatigue, mood changes, weight gain, and irregular cycles. I evaluate:
TSH — the primary screening test for thyroid dysfunction
Free T4 — to assess active thyroid hormone production
Total T3 — to evaluate thyroid hormone conversion and utilization
Bone Health
Bone loss accelerates significantly in the years surrounding peri/menopause due to estrogen's role in maintaining bone density. Early identification of osteopenia or osteoporosis allows for timely intervention. I evaluate:
Bone Density Scan (DXA) — to screen for osteopenia and osteoporosis
Comprehensive Metabolic Panel — including calcium, albumin, and phosphorus
Vitamin D — deficiency is extremely common and directly impairs calcium absorption and bone mineralization
PTH (Parathyroid Hormone) — elevated levels can drive bone loss, sometimes silently
Magnesium — plays an underappreciated role in bone health and vitamin D activation
Alkaline Phosphatase — a marker of bone turnover and liver function
Liver Health
Hormone changes, weight shifts, and fatty liver or metabolic associated liver disease becomes more common. I evaluate:
Liver Function Panel — to establish a baseline and screen for fatty liver disease or other hepatic conditions, which increase in prevalence after menopause
Platelet Count- This combined with liver function panel allows me to calculate the risk of someone having liver scarring
Metabolic Health and Insulin Sensitivity
Insulin resistance increases during the menopausal transition, raising the risk of type 2 diabetes and metabolic syndrome. I evaluate:
Hemoglobin A1c — reflects average blood sugar over the past 2–3 months and to scree for prediabetes and diabetes
Fatigue
Fatigue is one of the most common complaints during the menopausal transition and is often multifactorial. Before attributing it solely to hormonal changes, I screen for:
Ferritin — the most sensitive marker of iron stores, often low in women with heavy perimenopausal bleeding
Iron Panel — including serum iron, TIBC, and transferrin saturation
Vitamin B12 — deficiency is a frequently missed and treatable cause of fatigue, brain fog, and mood changes
The cardiovascular, thyroid, and metabolic labs listed above are also relevant here, as dysfunction in any of these systems can manifest as fatigue
Sleep Disturbance
Sleep disruption is nearly universal during the menopausal transition and can stem from hormonal changes, night sweats, mood disturbances, or independent sleep disorders. When a patient reports snoring, witnessed apneas, or non-restorative sleep, I pursue:
Sleep Study (Polysomnography) — to rule out obstructive sleep apnea, which is underdiagnosed in women and increases in prevalence after menopause. It is important not to assume all sleep complaints are hormone-related, as untreated sleep apnea carries significant cardiovascular and metabolic consequences

WHY WERE WE AFRAID OF HORMONE THERAPY FOR THE PAST TWO DECADES?
What CHANGED?
In the late 1980s, observational studies suggested that hormone therapy was beneficial for the prevention of coronary heart disease (CHD), dementia, and mortality. The American College of Physicians even advocated for the use of hormone therapy as a preventive strategy in 1992.
The issue was that observational studies showed only that hormone therapy was associated with reduced CHD—they did not prove that it caused the reduction. This became a critical question for the medical community. Thus began the effort to scientifically test a hypothesis that had generated significant excitement.
This led to the introduction of randomized controlled trials, which are designed to establish causation. In these studies, participants are randomly assigned to either an experimental or control group, eliminating choice and reducing confounding variables that could influence the results.
There were many studies conducted but the BIG one was the Women’s Health Initiative (WHI) conducted in 2002.
The Women’s Health Initiative
The women’s health initiative was the largest randomized controlled study ever performed for studying menopause.
There were two groups
16,608 women with a uterus were assigned to receive estrogen therapy with conjugated equine estrogen (CEE) along with a progestin, medroxyprogesterone (MPA).
10,739 women without a uterus received CEE alone, as progesterone is not required in the absence of a uterus.
In women with a uterus, progesterone is necessary to protect the uterine lining from excessive thickening caused by estrogen, which can increase the risk of endometrial cancer if left unopposed.
The results were unexpected and drew widespread attention. The CEE + MPA arm of the study was stopped early in 2002 due to an increased risk of pulmonary embolism (blood clots in the lungs), stroke, and invasive breast cancer, along with a non–statistically significant increase in myocardial infarction and coronary heart disease.
The CEE-only arm was discontinued in 2004 after an increased risk of stroke was observed.
The results were widely publicized before researchers had sufficient time to fully analyze the data and complete a thorough statistical evaluation. As a result, many physicians stopped prescribing hormone therapy, and patients abruptly discontinued their medications.
Since then, generations of physicians were not trained to treat menopause. It became a taboo topic, and when it was brought up, the response was often, “Remember the WHI?” Meanwhile, women continued to suffer.
Peri/menopause is not just about hot flashes—it affects mental health, sleep, and the ability to function day to day. Women demanded answers.
With the rise of social media and increasing independence, women began demanding answers.
This is the summary of what happened.
Pitfalls in the Women’s Health Initiative
Participants were not representative of the typical woman seeking treatment.
The Women’s Health Initiative focused on cardiovascular outcomes, so it primarily enrolled older women in their 60s who often did not have symptoms. This made it easier to study heart risk but did not reflect real-world patients—most women who seek care are in their 50s and looking for relief from symptoms.
Participants were outside the “window of opportunity”
Studies show hormone therapy has a better safety profile when started within 10 years of menopause and a less favorable profile when started more than 20 years later. In the WHI, the average age was 63.
For example, in relation to cardiovascular disease, women in their 60s are more likely to have established arterial plaque. In this context, estrogen may influence coagulation and vascular remodeling and increase metalloproteinase activity, which can weaken the fibrous cap of arterial plaques, potentially leading to plaque instability and rupture.Thereby, an increased risk of cardiac events was observed. In younger women without plaque, the effect can be anti-inflammatory or neutral. Timing matters!
Likely underpowered for subgroup analysis
Only 30% of participants were under age 60, making it difficult to draw conclusions about how hormone therapy affects women within 10 years of menopause.
Data interpretation
The results of the study were announced before careful statistical analysis was made. Risk was inflated and benefits underestimated. For example, there was a noted increased relative risk of breast cancer by 26%. However, this figure was widely misinsterpreted. People erroneously read that there was a 26% increased chance of developing breast cancer from hormone therapy. However, this is where absolute vs. relative risk is important to understand.
Relative risk describes how much more likely an event would occur in the group that received treatment compared to that which did not receive it. For rare events, the relative risk can inflate risk. For example, if the risk of something occurring is 2/10,000 and the risk increases to 4/10000 that is a 50% increase in risk!
Absolute risk tells you actual probability of an event occurring-the raw numbers. The absolute risk increase for breast cancer in the WHY was 8 out of 10,000 women. A very different perceived risk! Furthermore, the results were not statistically significant.
To compare what 8/10,000 increased risk is similar to:
To compare, a woman who has 2 glasses of wine each evening is taking on an increase relative risk of 18% and no one stopped allowing wine.
BMI above 28 (overweight) causes a 30% increased relative risk for breast cancer.
Having dense breasts causes a doubling of risk of breast cancer if there is scattered fibroglandular tissue and a 4 times risk for very dense breasts.
As you can see, when we compare the relative risks of being a human being rather than a size 0 barbie, there are environmental or other metabolic factors that portend a similar risk of developing breast cancer.

Understanding the risks and benefits of hormone therapy

Heart Health
First, lets discuss what the WHI taught us.
For my lecture on hormone therapy and heart disease to Endocrinology fellows, please click here.
What were the overall results?
In the Women's Health Initiative, women taking a specific type of hormone therapy (CEE + MPA) appeared to have a 18% higher relative risk of heart attack.
But when you look at the actual numbers, it was only about 6 extra cases per 10,000 women per year—and this finding was not statistically significant.
In simple terms: we can’t say for sure the therapy truly increased risk.
This is a good example of how risk can sound scary depending on how it’s presented.
What about younger women?
Women who were within 10 years of menopause on CEE+ MPA (combined therapy) actually showed a trend toward lower heart risk (but this was not statistically significant).
What did the study find for women ages 50–59 on estrogen alone?
After about 13 years of follow-up, younger women who took estrogen alone had significantly lower rates of heart problems compared to women who took a placebo (sugar pill):
Heart disease overall: About 34% lower risk
Heart attacks: About 40% lower risk
Need for heart procedures (bypass surgery or stents): About 44% lower risk
These results were statistically significant, meaning they were unlikely to be due to chance.
What about older women?
Women who started hormone therapy at age 70 or older had a higher risk of heart-related problems.
In women taking combined estrogen + progestin, the risk of heart attack was about 46% higher. This equals roughly 19 extra cases per 10,000 women per year.
In a later analysis of women 70+ with hot flashes, the risk was even higher—about 2 to 3 times greater risk of heart and blood vessel problems, including heart attacks and strokes.
Women who started hormone therapy 20 or more years after menopause also showed higher risk:
With combined therapy, heart disease risk was about 66% higher.
With estrogen alone, risk was about 12% higher, but this was not strong enough to be conclusive.
Why Does This Happen?
The leading theory is that by the time a woman is 70 or 20+ years past menopause, her blood vessels may already have plaque buildup (hardening of the arteries). Starting hormones at that point may destabilize those plaques or promote blood clots, rather than protect the heart.
In contrast, when hormones are started closer to menopause (within 10 years), the blood vessels are healthier and may respond more favorably.
THE TIMING HYPOTHESIS
These data led to what is known as the timing hypothesis.
It suggests that hormone therapy may have beneficial or neutral effects when started within 10 years of menopause or before age 60.
In contrast, starting hormone therapy later in life may be associated with neutral or potentially harmful effects.
Importantly, this does not mean hormone therapy cannot be started safely after 10 years from menopause—it simply means the risks and benefits may be different and should be evaluated individually.
Summary: Hormone Therapy and Heart Health
Overall, hormone therapy has a neutral effect on heart risk
There is an increased risk for women starting hormone therapy at ≥ 70 years of age.
For women within 10 years of menopause there may be a benefit to neutral effect of hormone therapy on cardiac risk.

DEMENTIA RISK AND COGNITION
Estrogen helps protect the brain by reducing inflammation, supporting brain cell growth, and helping the brain use energy efficiently. It also helps clear harmful proteins linked to Alzheimer's disease.
After menopause, estrogen levels drop. This can lead to reduced brain energy use, more inflammation, and a buildup of the same harmful proteins seen in early Alzheimer's disease.
These findings suggest estrogen may help preserve brain function, and hormone therapy could play a role in Alzheimer’s prevention when used appropriately.
The Women's Health Initiative Memory Study included women aged 65–79 who were not diagnosed with dementia.
It found:
A higher risk of probable dementia in women taking combined therapy
A non-significant trend toward increased risk with estrogen alone (CEE)
However, long-term follow-up (18 years) showed:
A 26% reduction in Alzheimer’s-related deaths in women who used estrogen alone
No clear effect in the combined therapy group
This was the only large study of its kind looking at hormone therapy and dementia risk in a randomized, placebo-controlled way
There are several important criticisms of these results
It measured overall dementia, not specifically Alzheimer’s disease.
The increase in risk was small in real numbers (about 23 extra cases per 1,000 women over 5 years)
The study included older women who started hormone therapy later in life, so results may not apply to women who start closer to menopause.
It only studied one type of hormone therapy (CEE ± MPA), so the results may not apply to other commonly used options like estradiol or micronized progesterone
Hormone Therapy & Dementia — What the research shows
The research on hormone therapy and dementia is not consistent, meaning studies do not all show the same results.
The effects of estrogen may vary depending on:
The type of hormone therapy
How it is taken (pill, patch, etc.)
A person’s overall health and genetics
Most studies looked at overall dementia, but different types—like Alzheimer’s disease vs. vascular dementia—may be affected differently.
Researchers also suggest two important ideas:
Timing matters: estrogen may be more helpful when started closer to menopause
Brain health matters: if brain changes are already present, estrogen may not help as much and could potentially have negative effects
Ultimately, we need more research in this area.
Research on hormone therapy and dementia risk is mixed and not fully settled.
Starting hormone therapy close to menopause appears to have a neutral to possibly protective effect on brain health. Starting it many years after menopause (age 65+) may carry more risk, especially with combined estrogen-progestin therapy.
This does not mean hormone therapy cannot be started at age 65 or older — but it does mean a careful, individualized conversation with your doctor is important. The type of therapy, the timing, and your personal health history all matter.

Bone Health and Hormone Therapy
Women can lose bone faster during the menopause transition.
Before menopause, bone loss is slow—about 0.1% per year. But around menopause, it speeds up:
In the 2 years before the final period: about 1.5–2.5% bone loss per year (spine)
In the 2 years after: peak loss of about 2.5–3.3% per year (spine)
After that: slows to about 1% per year, but continues
Overall, women may lose about 10% of spine bone density and 9% of hip bone density over the menopause transition.
Estrogen helps protect bone. When estrogen drops, bone loss accelerates.
In the Women's Health Initiative, hormone therapy reduced fracture risk (hip, spine, and wrist) by about 20–35%.
However, this benefit only lasts while taking therapy—once stopped, bone loss resumes.
Hormone therapy is approved for the prevention of osteoporosis. I strongly recommend this as a preventive strategy.
In summary, hormone therapy can prevent bone loss and osteoporosis.
Weight
A really common worry I hear is that hormone therapy causes weight gain, but the research just doesn’t support that.
After menopause, it’s normal for women to gradually gain weight and, more importantly, to notice a shift in fat from the hips and thighs toward the abdomen. That “belly fat” (visceral fat) is the type most closely linked with heart disease and diabetes.
What the studies show is actually pretty reassuring. A large Cochrane review found that hormone therapy does not cause extra weight gain beyond what normally happens with menopause. In big studies like the Women's Health Initiative and the PEPI trial, women on hormone therapy actually gained a little less weight over time (about 2 pounds less over 3 years) and had less increase in waist size. There was also some preservation of muscle mass and less of that shift toward abdominal fat.
Women who are currently on hormone therapy tend to have slightly lower belly fat and BMI, but those benefits go away once the therapy is stopped. Even combinations like estrogen with micronized progesterone generally show no weight gain, and may slightly help blunt some of the body composition changes that come with menopause.
In Summary:
Hormone therapy does not cause weight gain. If anything, it may modestly help with the normal midlife shift toward abdominal fat—but it’s not a weight loss treatment.

INSULIN RESISTANCE AND DIABETES
After menopause, lower estrogen can make it easier to gain belly fat and can also affect how the body handles sugar. This can lead to higher blood sugar and more insulin resistance, which over time increases the risk of type 2 diabetes.
In the Women's Health Initiative, there was actually a lower risk of developing diabetes in women taking hormone therapy:
The combined estrogen + progestin group had about a 19% lower risk
The estrogen-only group had about a 14% lower risk
These results were statistically significant, meaning they are unlikely to be due to chance. The effect did go away after stopping therapy, though.
When we look across multiple studies, hormone therapy also seems to help the body respond better to insulin. In women who already have diabetes, it may even help modestly improve blood sugar control and lower HbA1c.
That said, hormone therapy is not prescribed to prevent diabetes—this is more of an added benefit we see in women who are already taking it for menopausal symptoms.
In summary: Hormone therapy appears to have a favorable effect on blood sugar and insulin sensitivity, especially while it is being used.
CLOT RISK
In the Women's Health Initiative, oral hormone therapy (taken as a pill) was linked to a higher risk of blood clots. With combined therapy, headlines often reported a “100% increase in risk,” which refers to relative risk. In absolute terms, this translated to about 9 extra blood clot cases per 10,000 women per year. Estrogen alone showed a smaller or less clear increase in risk.
The increased risk was mostly seen early—within the first 1–2 years of use—and it decreased over time, going away after stopping therapy. For women ages 50–59, the absolute risk increase was very small.
What we understand now is that blood clot risk depends a lot on the type and route of hormone therapy.
Pills (oral estrogen) go through the liver first, which is where the clotting risk seems to increase
The higher risk in WHI was mainly linked to oral estrogen + synthetic progestin (MPA)
In fact, MPA itself appears to increase clot risk
In contrast, newer options look different:
Transdermal estrogen (patches, gels, sprays) does not appear to increase blood clot risk because it bypasses the liver
Micronized progesterone (natural progesterone) also does not appear to increase clot risk
Overall, current evidence suggests that transdermal estrogen combined with micronized progesterone is likely the lowest-risk option for blood clots, especially compared with older oral formulations.
In summary: Blood clot risk is largely solved by using transdermal estrogen and micronized progesterone
Stroke Risk
Stroke risk was also evaluated in the Women's Health Initiative. Both combined hormone therapy and estrogen alone were associated with about a 35% relative increase in stroke risk, which translates to roughly 9 extra strokes per 10,000 women per year. This increased risk went away after stopping therapy. In women ages 50–59, the absolute number of extra strokes was very small and not statistically significant.
What we understand now is that stroke risk is more complex than blood clot risk and may not be fully eliminated by changing formulations. However, how hormone therapy is given and which type of progesterone is used both seem to matter:
Estrogen delivered through the skin (patches, gels, sprays) — especially at low doses — appears safer for stroke than estrogen taken as a pill. Lower-dose patches (≤50 mcg) do not appear to significantly increase stroke risk, although the evidence is less definitive than for blood clots.
Natural progesterone (micronized progesterone) does not appear to increase stroke risk.
The synthetic progestin (MPA) used in the WHI study was linked to higher stroke risk, though it was always used with oral estrogen pills, so it is hard to know how much of the risk came from MPA alone.
Overall, stroke risk is most relevant in women who are older or who already have risk factors such as high blood pressure, smoking, or diabetes. In younger, healthy women near menopause, the absolute risk remains very low.
In summary, the risk of stroke with hormone therapy is very low.
Gastrointestinal Cancer
One of the more reassuring findings from hormone therapy research is that it does not appear to increase the risk of digestive cancers, and may even have some protective effects.
For colon and rectal cancer, the Women's Health Initiative initially showed fewer cases in women using combined hormone therapy. However, with longer follow-up (up to 24 years), that early benefit became less clear. Even so, many large studies overall suggest about a 15–35% lower risk of colon and rectal cancer in women who have used hormone therapy compared with those who have never used it.
That said, hormone therapy is not prescribed to prevent colon cancer—this is just an observed association.
For stomach and esophageal cancers, research also suggests a possible protective effect. Women who use hormone therapy appear to have about a 20–30% lower risk, and longer duration of use may be associated with greater reduction in risk.
A possible explanation is that estrogen receptors are present throughout the digestive tract, and estrogen may help protect the lining of the stomach and intestines from long-term damage.
To summarize: Hormone therapy appears to have a neutral to potentially protective relationship with digestive cancers, which is reassuring, even though it is not used specifically for cancer prevention.
Mortality
One of the most reassuring things we’ve learned from hormone therapy research is actually pretty simple: it does not increase the risk of dying.
In the Women's Health Initiative, women who took hormone therapy had the same overall death rate as women who didn’t take it — meaning no increase in deaths from heart disease, cancer, or anything else.
Even more interesting, when we look at women in their 50s (closer to menopause), some analyses actually show a lower risk of death during treatment. For older women starting later in life, that benefit wasn’t seen, which really highlights that timing matters.
Other large studies show a similar pattern. Some real-world data even suggests that women who used hormone therapy for several years had a slightly lower overall death rate, and this is especially true when it’s started closer to menopause or in women who had early loss of estrogen.
In summary:
Hormone therapy does not increase mortality risk. In some women—especially those closer to menopause—it may even be linked with a small survival benefit. The key factor that keeps coming up across studies is timing
Breast Cancer Risk
Understanding the Breast Cancer Risk Numbers
When the WHI results first came out, headlines said hormone therapy increased breast cancer risk by 26%. This number was widely misunderstood. Many people read this as a 26% chance of getting breast cancer — but that is not what it means. The actual increased risk was 9 extra breast cancers per 10,000 women per year — or less than 1 in 1,000.
To compare what 9 in 10/000 increase in risk is, lets compare it to the risks of everyday factors that many women already live with:
Having 1–2 glasses of wine most evenings is associated with about a 10–22% higher relative risk of breast cancer.
Being overweight after menopause is linked to a clearly higher risk of breast cancer, especially the hormone-sensitive (estrogen-receptor positive) type.
Having dense breasts can increase breast cancer risk about 2 times with moderate density and up to 4 times with very dense breasts.
When you look at it this way, the small absolute increase seen with hormone therapy sits in the context of many common, everyday risk factors that are often not thought of in the same way.
The type of hormone therapy matters
Not all hormone therapy is the same.
Estrogen alone (for women without a uterus): These women had a 22% lower risk of developing breast cancer and a 40% lower risk of dying from breast cancer.
Combined therapy (for women with a uterus):
Small increase in risk seen mainly with an older synthetic progestin (MPA), which we do not commonly use nowadays
There was no clear increase in breast cancer deaths, and the trend toward higher mortality was not statistically significant. After stopping therapy, the increased risk gradually went down over time.
The type of Progestin matters
More recent research suggests that micronized progesterone (a body-identical form) does not appear to increase breast cancer risk in the same way as synthetic progestins like MPA. Large studies showed no increased risk with micronized progesterone in the first 5 years.
My advice is really simple—stay on top of your regular breast cancer screening, try to eat well, and keep your body moving. Those things make a much bigger difference to overall health than the very small risk we see with hormone therapy.
And honestly, for a lot of women, hormone therapy is what helps them sleep better, feel more like themselves, and actually have the energy to take care of their health in the first place.
So when I look at the big picture, for the right person, the benefits by far outweigh the risks.
To Summarize:
The breast cancer risk with hormone therapy is often overstated in headlines.
For most women,
The absolute risk increase is very small
Estrogen alone is actually reassuring or possibly protective
Combined therapy has a small increase in risk, mostly related to older synthetic progestins
The type of progesterone really matters

Vaginal Dryness
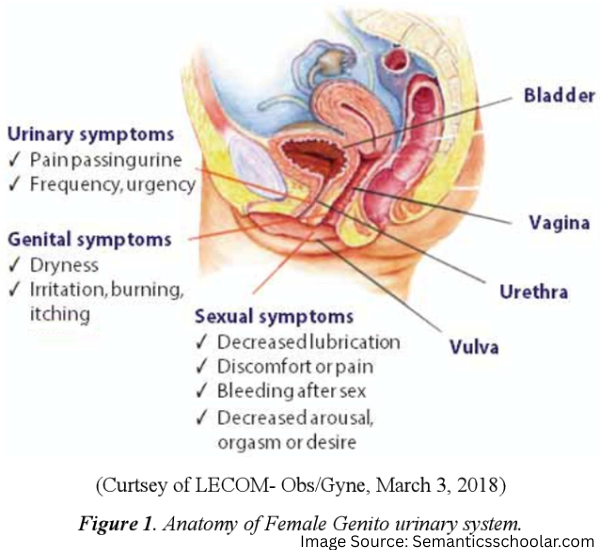
During perimenopause and menopause, your estrogen levels drop. This affects your vaginal and urinary health in several ways—a condition doctors call "genitourinary syndrome of menopause (GSM)."
Common changes you may notice:
Vaginal and vulvar dryness: Lower estrogen causes the tissues in and around your vagina to become thinner and less moist. Atrophy of the vulva and vagina can occur. This can lead to discomfort, itching, or pain during sex.
Increased urinary tract infections: As vaginal dryness develops, the normal balance of healthy bacteria changes and the vaginal pH increases. These changes make it easier for urinary infections to develop.
Bladder symptoms: Your bladder also has estrogen receptors, so lower estrogen levels can cause symptoms like sudden urges to urinate or needing to go more frequently (overactive bladder).
Sexual Symptoms: You may experience decreased lubrication, pain or bleeding during intercourse, reduced sexual desire, or less pleasurable sensations during intimacy. These changes can affect your comfort and satisfaction with sexual activity.
Women are being undertreated…and this needs to change!
Around 50% of postmenopausal women experience symptoms of GSM, yet only 6–7% receive treatment.
Women often think this is just a normal part of aging or feel embarrassed to discuss genital or sexual concerns. You do not have to suffer from vaginal dryness—it is treatable.
Please note that other conditions can mimic GSM, so a pelvic exam is important to confirm the diagnosis.
“Unlike hot flashes, this condition worsens with time and needs to be treated. Regardless of your age or medical history, you do not have to suffer since numerous safe treatment options are available.”
Treatment Options
There are many hormonal and non-hormonal treatment options, each with different mechanisms and ways of being administered. The options are extensive, so if one approach isn’t effective for you, your doctor can help you explore other safe alternatives.
Environmental:
Avoid irritants: Women may develop local irritation from products like soaps, laundry detergents, or sanitary pads. I recommend wearing cotton underwear and avoid pads, panty liners, and scented materials. If irritation occurs, try a warm sitz bath followed by gently patting the area dry and applying an emollient, such as Aquaphor (petrolatum).
Regular sexual stimulation: It promotes vaginal blood flow and natural lubrication. This can be achieved with a partner, on your own, or with the use of a vibrator. However, women who experience pain with intercourse should focus on healing the vaginal tissue first, as penetration may be uncomfortable or even traumatic.


“Use it or lose it” is just wrong and inconsiderate.
Why can a vibrator be your best friend?
A vibrator can stimulate the clitoris—the primary center of arousal in women. This increases blood flow to the pelvic area and helps the pelvic floor muscles relax. Together, these effects can support pelvic floor health.
You can consider using a vibrator for a few minutes a day. Remember, it is a tool, not a toy. If you end up achieving an orgasm, this is an added benefit!
Pelvic Floor Physical Therapy: Even after treating vaginal dryness and the vaginal tissue heals, women may still experience pain with sex or myofascial pelvic pain syndrome. This is because their muscles tighten up as a protective mechanism to pain. This is where a pelvic floor physical therapist can help relax these muscles allowing for sexual activity to be possible and enjoyable. Pelvic floor physical therapy can also strengthen weak pelvic floor muscles.
Non-Hormonal Remedies:
Vaginal Moisturizers: use this regularly a few nights per week to maintain moisture
Replens
HydroGyn
Vaginal moisturizers with hyaluronic acid:
Good clean love bioNourish
Hyalo Gyn
Revaree
Vaginal Lubricants: use prior to sexual activity to reduce friction
Astroglide X*
FemGlide
Good Clean Love
Lush*
Sliquid Organics*
UberLube*
*Silicone-based lubricants last longer than water-based ones, but they should not be used with silicone sex toys. Oil-based lubricants may damage condoms and increase the risk of vaginal infections.
Natural products:
Inexpensive options include baby oil, mineral oil, petroleum jelly, olive oil, coconut oil but these can clog pores and cause breakouts.
Hormonal Options:
Vaginal Estrogen
Vaginal estradiol products do not raise blood estrogen levels beyond what is normal for a postmenopausal woman. They do not increase the risk of breast cancer, clots, strokes, or heart attacks. These products are safe at any age, but should be avoided in cases of uterine cancer or unexplained vaginal bleeding.
Vaginal estrogen DOES NOT increase the risk of recurrence of breast cancer. This is well described in literature. A nuanced conversation is needed for women on estrogen deprivation therapy for a history of breast cancer.
FDA approved vaginal estrogen treatments
Vaginal cream: 0.5-1 gm 2-3 x/ week
Vaginal ring: 7.5mcg every 3 months
Vaginal tablet: 10mcg 2x/ week
Vaginal insert: 4mcg or 10mcg 2x/ week
The vaginal cream is excellent because it can be applied to the vagina, introitus and vulva. However, all options are effective.
How to apply: Many women find the vaginal estrogen applicator irritating. Instead, wash your hands and apply a fingertip of vaginal estrogen cream at lower ⅓ of vagina, vulva and introitus.
Additional Hormonal Products
Vaginal DHEA (Intrarosa): FDA approved to use daily. Improves sexual function, vaginal dryness, pain with sex & does not increase estrogen levels in the body at all. This can be a good option for a woman with a history of breast cancer.
OSPEMIFENE: Selective estrogen receptor modulator. This is taken orally. Best for women who prefer not to apply estrogen vaginally and have a high risk of breast cancer. There is a very small risk of clots.
Vaginal Testosterone: It is a compounded product, so dosing can be inconsistent. There are no high-quality randomized controlled studies supporting its use yet.
INFORM YOUR CLINICIAN IF YOU HAVE ANY POSTMENOPAUSAL BLEEDING.
Recurrent Urinary Tract Infections and Urgency
Chronic vaginal dryness can increase the risk of urinary tract infections over time. Many women experience recurrent infections and are treated repeatedly with antibiotics.
Vaginal estrogen can reduce the risk of recurrent urinary tract infections by up to 58%. Oral estrogen does not provide this benefit—local therapy is necessary. The American Urological Association recommends vaginal estrogen for the prevention of recurrent UTIs.
Estrogen receptors are also present in the bladder and urethra. As a result, urinary symptoms may include urgency, frequency, nighttime urination, pain with urination, burning, and itching. Vaginal estrogen can help improve these symptoms.
Laser Rejuvenation
Why I Don’t Recommend Vaginal ‘Rejuvenation’ Treatments
I discourage this approach. Many clinics and spas market these treatments — often referred to as “vaginal rejuvenation.”
A randomized controlled trial (FG et al., doi:10.1001/jamanetworkopen.2022.55697) found no difference in symptom improvement between a probe without laser and one with laser.
The FDA has issued warnings against the use of energy-based devices for “vaginal rejuvenation” or other cosmetic procedures. These treatments carry risks, including scarring, vaginal burns, and chronic pain.
They are also costly, with no proven benefit.